65 M with sudden onset chest pain.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comments
A 65 old Retiered security guard and farmer presented with complaints of sudden onset chest pain since 6 hours associated with sweating.
Patient was apparently normal 35 years back, later he had an penetrating injury to left eye, while he was cutting wood small piece of wood penetrated in his left eye following which he used some herbal medication (applied on eyes), end up in blurred vision.
30 years back he had a History of fall (from vehicle) following which he had Right eye injury
Patient currently using HOMATROPINE BROMIDE Since 15-20 years. Attenders claims that he use eye drops to make his vision clear. If he didn’t use eye drops he then have blurring of vision.
Patient developed chest pain @ 4.30pm on 18\1\2021 which is sudden is onset ,progressive ,radiating to both shoulders with Epigastric discomfort. He went to physician in suryapet where he ordered an ECG which shows ST elevations in V2to V4, lead 1 and avL and diagnosed with ANTEROLATERAL WALL MYOCARDIAL INFARCTION

and gave Him inj. FONDAPARINOX 2.5MG IV STAT, TAB.CLOPIDOGREAL 75MG PO STAT, TAB.TELMISARTAN 40MG STAT,TAB.AMLODIPINE, and referred to us for thrombolysis.
Patient presented to ER ( Dr. Nikitha pgy2 ) around 11.00pm with mild chest discomfort ( after taking medications)
Initial ECG recordings were obtained and troponin-I was positive.

INITIAL ECG SHOWS : PROXIMAL LAD GRADE 2 STEMI (V2,V3, V4, 5, V6 L1 AVL)
TIME OF ONSET OF CHEST PAIN TO PRESENTATION IS ROUGHLY 7 HOURS.
Planned for medical thrombolysis with streptokinase
Indications : Ongoing chest pain and Evolving MI.
NO Absolute contraindications present like :
No H/O Hemrrhagic / ischemic stroke
No H/o GI bleed
PRE-PROCEDURE ECGS
Pre-procedure vitals :
Bp-150/100mmhg
PR- 82bpm
RR - 20cpm
spO2 - 94% with room air
GRBS 100mg/dl
Thrombolysis started with INJ. STREPTOKINASE 1.5M units IV over 90 min was given (due to technical issues) During thrombolysis patient had occasional left ventricular VPC’s, junctional rhythms& AIVR for a few seconds.
Serial ECGS :
Outside hospital

Base line ECG @ presentation to ER: (11.00pm)
ECG1 :
15 min After thrombolysis: ECG 2 @ 12.10am

1 hour after initiation of thrombolysis: ECG 3 @12.55am

ECG IMMEDIATELY AFTER THROMBOLYSIS ECG 4 @ 1.25am

Serial ECGS were taken which showed significant STE reduction along with T wave inversion.
Patient didnot developed any complications.
Post procedure vitals :
BP - 120/80mmhg
PR - 67bpm
RR - 14cpm
spO2 - 96% on room air.
Overall procedure was uneventful.
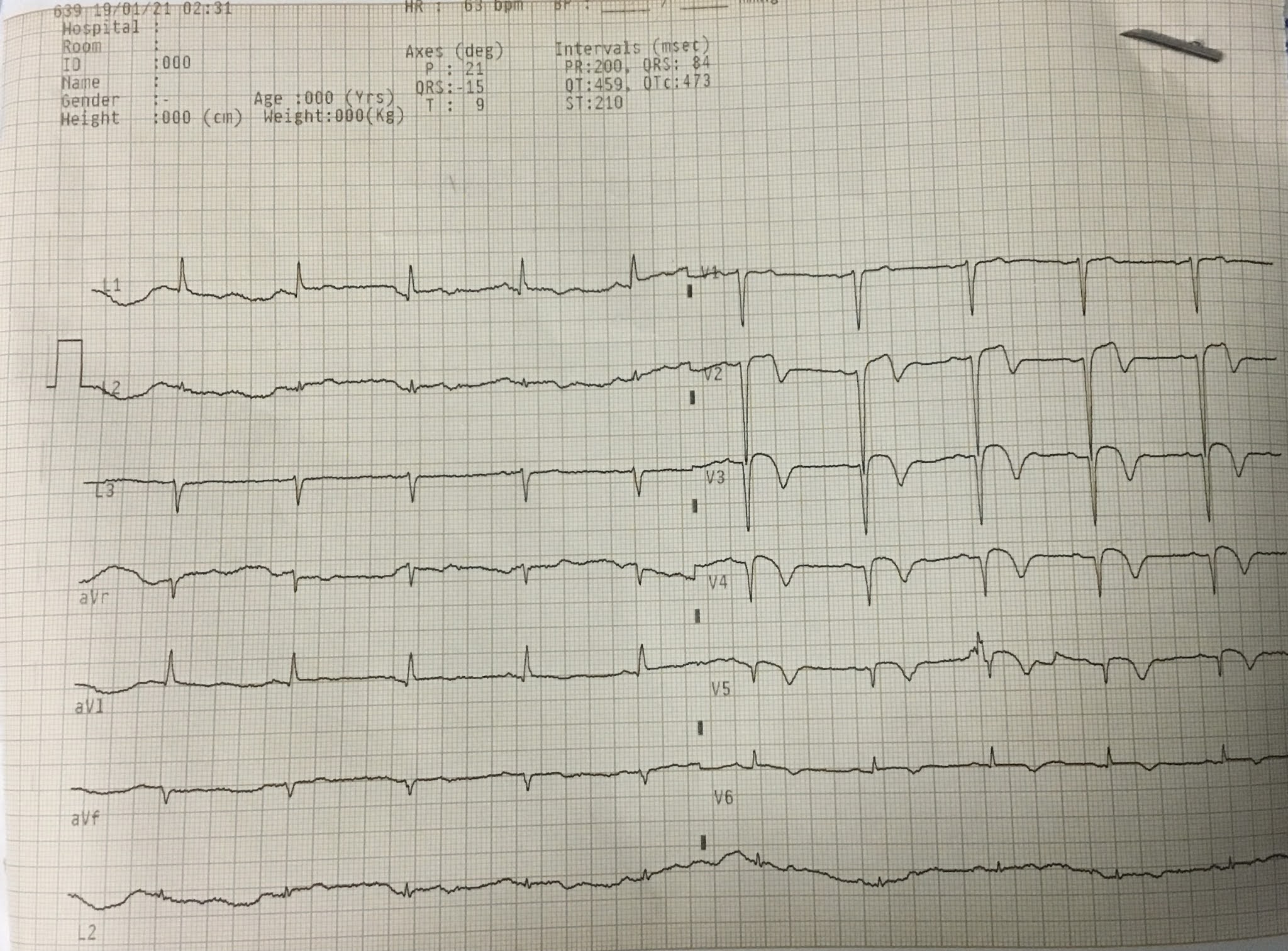
1hr post thrombolysis ECG 5 @ 2.30am
Labs ;
Hemogram

PT- 18sec
INR- 1.33
APTT- 35sec
BT - 2.30 MIN
CT - 4.30 MIN
TROPONIN-1

Treatment Given :
TAB. MET-XL 50MG STAT
TAB. ATROVASTATIN 80MG STAT
INJ. STREPTOKINASE 1.5 MILION UNITS IN 50ML/hr
BP,PR,SPO2 , MONITORING.
THANK YOU UNIT-1 TEAM, DR.NIKITHA (DMO), Dr. K. Vaishnavi (ICU).



Comments
Post a Comment